Barriers to Opening an OTP
Author

Media Contact
For general and media inquiries and to book our experts, please contact: pr@rstreet.org
Methadone is a lifesaving medication used to treat opioid use disorder (OUD). More than 50 years of evidence demonstrates that methadone reduces overdose risk (recent studies indicate by as much as 80 percent) and non-medical use of opioids. Taking methadone as treatment for OUD improves individuals’ lives—including their ability to hold a job and engage in healthy relationships with family and loved ones—and reduces criminal activity.
Nonetheless, in the United States, methadone for the treatment of OUD is only available in opioid treatment programs (OTPs), commonly known as “methadone clinics.” One factor that deters many current and potential OTP patients from engaging with their treatment is the common mandate that patients visit the clinic in person several times per week or more to receive their medication under supervision. This requirement interferes with work and personal obligations, in large part due to excessive travel times. The United States lacks enough OTPs to meet treatment needs for people with OUD, and the clinics we do have are disparately distributed, hindering access to care and preventing patient choice.
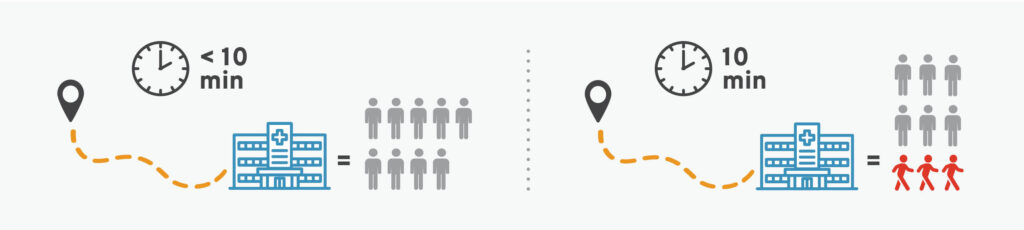
In fact, the average travel time to an OTP is about 45 minutes one way. This is particularly troubling since a commute time of just 10 minutes has been shown to cut treatment retention by 33 percent.
Therefore, one way to combat the nation’s persistent overdose crisis would be to improve geographic access to OTPs. But solving this problem is not as simple as it seems. Unfortunately, many barriers prevent organizations from opening new OTPs.
Federal Requirements
Under federal guidelines, OTPs must be accredited by an approved body, certified by the Substance Abuse and Mental Health Administration, and registered with the Drug Enforcement Administration (DEA). These certifications and registrations hold OTPs to certain standards that can be costly and complicated to meet. For example, the DEA requires OTPs to take special precautions when storing methadone, mandating locking safes or steel cabinets—at least 750 pounds or attached to the floor—for small quantities and, for larger amounts, vaults secured with an alarm system. Installing these and other security measures is a costly endeavor. OTPs must also keep thorough records—not just on patient treatment, but on the storage, dispensing, and disposal of medications as well. Federal organizations and accrediting bodies verify compliance with these requirements via site visits, adding time and logistical obligations to the already challenging task of opening an OTP.
State Laws
In addition to federal regulations, OTPs must be licensed by their states and follow state and local laws. And to some degree, every state regulates OTPs and the use of methadone for OUD treatment more strictly than the federal government does. A number of these regulations target the facilities themselves.
For example, many states place geographic restrictions on OTPs. This includes limiting the total number of OTPs allowed in the state or in a region or enacting zoning restrictions that prohibit OTPs near other treatment facilities or schools. Another way states hinder the opening of new OTPs is by requiring evidence of need or approval from local government or relevant local agencies. Some states also limit OTPs by placing difficult-to-meet restrictions on their operations. For example, requiring OTPs to receive pharmacy licensure and/or to have a pharmacist on-site can increase costs and paperwork burdens without improving quality of care.

Why It Matters
The above restrictions are often intended to improve quality of OUD treatment and to protect communities by preventing the diversion of methadone to the illicit market. But they frequently have unintended consequences. By making it difficult to open new OTPs, state and federal governments perpetuate the limited and disparate access to evidence-based OUD treatment in the United States. In turn, there is a risk of poorer health outcomes for people with OUD, including overdose. In fact, research has found that states with more OTP regulations have more opioid-related deaths and emergency room visits.
Lawmakers can help solve this problem by addressing regulations that prevent the opening of new OTPs. Facilitating the proliferation of these clinics would, at a minimum, improve basic access to OUD treatment, especially in underserved areas. And if enough OTPs were to open, they could create competition for one another, challenging the current monopoly-like framework and improving patient care.