An Ever-Changing, Increasingly Toxic Drug Supply Makes Harm Reduction Essential
Authors

Table of Contents
- Executive Summary
- Introduction
- The Public Health Burden of Illicit Markets
- Adulterants in the United States
- Harm Reduction Policy and the Evolving Supply
- Conclusion
Media Contact
For general and media inquiries and to book our experts, please contact: pr@rstreet.org
Harm reduction directly empowers people who use drugs to stay safer and healthier, especially when policy allows programs to be tailored locally and in real-time.
Executive Summary
In the United States, annual drug overdose deaths have been rising rapidly for the past decade, peaking at more than 111,000 in 2022 before falling to about 90,000 last year. This crisis is largely driven by the illicit drug supply, which is marked by inconsistent drug purity and quality, ever-increasing drug potency, and a general lack of product transparency. While the illicit drug supply has always posed these risks to some extent, the growing capacity to produce synthetic drugs amplifies them by incentivizing the emergence and proliferation of an evolving variety of even more potent adulterants that heighten and complicate overdose risk, as well as introduce new health threats.
This policy study examines the evolving nature of the illicit drug supply throughout the last decade across the United States and highlights harm reduction interventions and relevant policies that can save lives. By looking at the evolution of adulterants—including illicitly manufactured fentanyl, the veterinary sedative xylazine, and several other novel opioids and sedatives—this study explains the supply-side dynamics that drive overdose risk. We demonstrate that the intersection of drug use and supply patterns shape the often-localized spread of adulterants.
Although the dangerous fluctuations in the availability, potency, and purity of the illicit drug supply are largely the result of supply-side factors, demand-side interventions can save lives. Harm reduction directly empowers people who use drugs to stay safer and healthier, especially when policy allows programs to be tailored locally and in real-time.
Introduction
Although people have been using psychoactive substances for as long as we have records, social norms—and in modern times, laws—often deem certain substances acceptable and others unacceptable, or even illegal. As we saw under alcohol prohibition, the criminalization of substances, while often well-meaning, can have unintended consequences that increase the risks associated with use. In fact, the dangers of the illicit market have become exceptionally clear in recent years. Annual drug overdose deaths have skyrocketed in the past decade, from 47,523 in 2014 to more than 111,000 in 2022. In the past year, that number has fallen to about 90,000. This overall increase in deaths is largely attributable to the emergence and proliferation of highly potent synthetic opioids such as fentanyl, which began as adulterants and have spread widely, even replacing heroin in some markets. The term “adulterant” primarily refers to substances that are “deliberately added to increase bulk, enhance or mimic a pharmacological effect, or to facilitate drug delivery.”
Recent reports indicate that overdoses may finally be plateauing or even declining in some populations and that the fentanyl supply may be decreasing in certain areas. However, statistics from the past 10 years demonstrate that the illicit supply is unlikely to become less lethal as a consequence of these changes, especially in the age of profit-friendly synthetic drugs that are easier to make (or alter to create something novel) than drugs derived from organic compounds. Indeed, fentanyl is not the first adulterant (the illicit market has always been adulterated), and a wide variety of potentially harmful substances have emerged or spread throughout the illicit market in recent months.
In this study, we discuss the reasons and ways that illicit drug markets contribute to a supply that endangers public health; trace the geographically and temporally specific emergence of fentanyl, xylazine, and novel adulterants throughout the country; and outline how policymakers wanting to better protect their communities from the dangers of the illicit supply can optimally implement harm reduction strategies.
The Public Health Burden of Illicit Markets
The concept that an illicit drug market fosters a dangerous supply and increases public health risk is not novel in U.S. history. Most Americans are familiar with the United States’ trial of widespread alcohol prohibition—which started with state and local bans during the early 1900s and culminated in federal prohibition from 1920 to 1933. Although prohibition may have driven down the number of drinkers in the nation, it created a market characterized by poor quality control, increasingly potent alcohol, a lack of consumer awareness about what they were consuming, and increased criminal behavior. For example, doctors saw a rise in unusual alcohol-related poisonings resulting from the consumption of “mixtures containing methyl alcohol and mixtures made from denatured alcohol.” We see these same types of challenges in the illicit drug supply today as drugs have become increasingly potent and the supply is contaminated with a growing variety of potentially toxic substances. Below, we explain how a lack of quality control, increasing potency, and a lack of transparency in the risks of using such products similarly contribute to the public health crisis around the illicit drug market.
Lack of Quality Control
The regulation of legal consumer products helps ensure that they are safe, effective, and appropriately portioned. This type of quality control, however, is not built into the illicit market, which can result in serious health consequences. For example, the 2019 e-cigarette or vaping product use-associated lung injury (EVALI) epidemic was linked to the use of “illicit, pre-filled THC vape cartridges” that contained vitamin E acetate, which, when aerosolized, resulted in lung injuries.
Similarly, illicit drugs are frequently adulterated or “cut” with substances unknown to the end consumer. Most often, these adulterants are other psychoactive drugs meant to boost or complement a high while cutting costs, or they are filler intended to dilute effects and stretch a supply. However, some can lead to serious health consequences, especially when unknowingly consumed alone or mixed with other substances. Thus, in the absence of regulations that would label ingredients or dosages, engaging with the illicit market is a game of roulette.
Increasing Potency
Research has shown that illicit markets incentivize manufacturers, traffickers, and distributors to put forth ever more potent substances—a concept often referred to as “The Iron Law of Prohibition.” Under alcohol prohibition, this led to a boom in liquor over beer. In today’s illicit drug market, prohibition has encouraged the production and sale of synthetics. These substances are more potent than their organic counterparts, which means they can be trafficked and sold in smaller quantities, making them easier to move and conceal. They are also more profitable to produce because they tend to be less labor-intensive, require less space (i.e., a laboratory rather than large swathes of land), and do not have a lengthy growing season.
Lack of Transparency
Illicit markets lack an important quality-control mechanism that is considered critical for consumer safety, awareness, and choice: transparency. Perhaps most importantly, the purity and potency of unregulated/illegal substances vary, and consumers have no way to know the chemical composition of the substances they intend to use before purchasing them. As such, they cannot ensure they are taking the intended dose, even if they have considerable experience using a particular substance. Indeed, fluctuating supply potency is a major contributor to illicit opioid overdoses. In addition, localized drug busts or seizures disrupt trusted supply chains and have been shown to precede jumps in the number of overdoses in the surrounding areas. This is likely in part because many people who use drugs depend on known suppliers as a harm reduction measure. When that safeguard is removed, consumers lose a layer of protection.
Adulterants in the United States
The U.S. illicit drug market has always been adulterated, as producers and sellers strive to bypass enforcement and maximize profit and do so unburdened by the need to follow health or safety regulations. Sometimes, particular adulterants emerge and remain isolated to specific populations or locations. Other times, we see particular adulterants emerge across multiple communities, although it can take years for an adulterant or new drug to spread across the country because of regional differences in drug use patterns, trafficking networks, and other factors. As such, the adulterants a person is exposed to and the consequent risks to their health and life vary both according to the substance used and the physical location of the drug acquisition. This section draws on reports and data from law enforcement seizures, overdose death records, and community and mail-in drug-checking services to describe the emergence and diffusion of two common adulterants—fentanyl and xylazine—as well as other emerging substances and to outline the current state of drug adulteration in the United States.
The Proliferation of Fentanyl
Fentanyl is a synthetic opioid that is as much as 50 times stronger than heroin. Pharmaceutically manufactured fentanyl is a fairly common painkiller and sedative used by medical professionals. However, illicitly manufactured fentanyl (IMF) and its analogs have been driving the U.S. overdose crisis for roughly a decade, contaminating a growing variety of street drugs, including heroin, methamphetamine, cocaine, and benzodiazepines. A potent opioid, IMF causes respiratory depression more quickly and at much smaller doses than many other opioids, including heroin. In this section, we trace fentanyl’s emergence and proliferation in illicit drug markets throughout the United States.
IMF began appearing in the U.S. drug supply in the early 2010s, driving the third wave of the nation’s overlapping overdose crises. Since the 1990s, increases in opioid use and overdoses in the United States have been driven by overprescribing—especially of novel pharmaceutical formulations that increased the risk of tolerance, dependence, and overdose—followed by knee-jerk overregulation that led providers to rapidly taper or outright refuse to continue prescribing opioid medications. This clampdown on prescription opioids drove many people to seek illicit opioids, creating a larger pool of people engaging with the illicit market.
Thus, when IMF came on the scene, its potency tragically compounded the dangers of the growing U.S. market for illicit opioids. The Northeast and Midwest were the first parts of the country to undergo what some have referred to as “fentanyl shock”—the rapid proliferation of IMF and increases in associated overdose deaths. Starting in 2014, overdose rates started to skyrocket in these states, and, soon after, the southern United States also began seeing the effects of IMF. In subsequent years, different parts of the country experienced this same fentanyl shock and saw their overdose rates spike. Figure 1 illustrates how fentanyl spread to the four U.S. regions at different times.
Figure 1: Regional Trends in Fentanyl Reported per 100,000 People Aged 15 or Older, January 2008 to December 2022
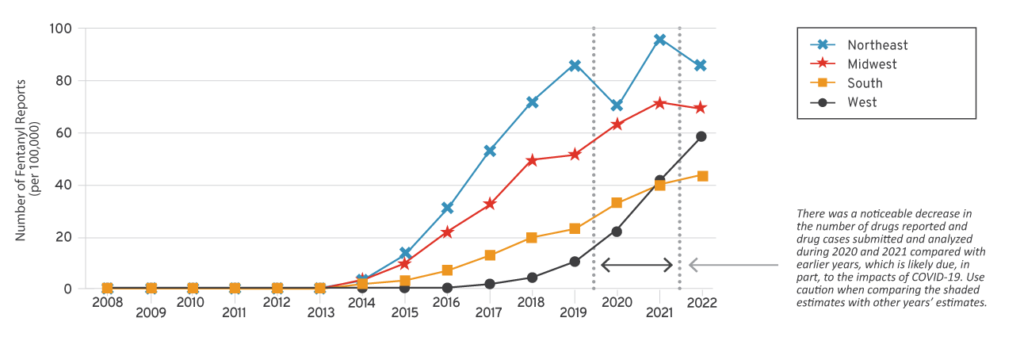
Fentanyl did not arrive in western states for several years. For example, California first saw a rapid rise in IMF seizures and related deaths in 2016 and 2017, and Oregon did not experience fentanyl shock until 2021.
The surge of IMF across the United States over the past decade appears to be driven by supply-side dynamics rather than demand-side factors. This aligns with the fact that, especially when IMF first came onto markets, it was sold as heroin. Indeed, in the years immediately following IMF’s 2014 emergence on the market, few people who use drugs (PWUD) sought out IMF, and many actively avoided the highly potent opioids. Even in more recent studies, many PWUD do not seek out and cannot consistently identify IMF in their supply. In fact, fentanyl continues to be sold as heroin in some markets, especially in the eastern United States. It is only very recently that states—especially in the western United States—have begun to see demand change such that people seek out IMF and there is more transparency around sales. These factors suggest that demand did not drive the emergence of IMF on the illicit market.
Three key supply-side dynamics are thought to have driven the erratic geographic spread of IMF across the United States:
- Localized shortages
- Individual states’ primary source country for illicit drugs
- The dominant type of heroin of each state’s illicit drug market
Some experts have argued that IMF emerged at the beginning of the third wave of the U.S. overdose crisis and spread across the nation in response to localized heroin shortages or declines in the quality or purity of heroin. This would be consistent with findings from past (brief) surges in the drug in U.S. markets as well as overseas. For example, a temporary drop in heroin purity in New Jersey in 2006 was associated with a spike in IMF-involved overdoses. However, this explanation is likely not the sole cause of the drug’s broader, but geographically staggered, spread.
Another contributing factor is thought to be the country of origin of different states’ supply. Drug trafficking source countries vary by region, change over time, and influence the specific drugs that dominate an area. Before 1980, most of the heroin in the United States came from southeast Asia, southwest Asia, and, to a smaller extent, Mexico. Colombia entered the market in the 1990s and provided almost half of all U.S. heroin by 2000. Around the same time, Asian-sourced heroin began to decline—falling to about 10 percent in 2000 and just 2 percent by the mid-aughts—and Mexico became a significant source country, supplying about 40 percent of U.S. heroin. Thus, in the decades leading up to IMF’s surge onto the illicit U.S. drug market, the vast majority of illicit opioids (primarily heroin) came from either Colombia or Mexico, with Colombian heroin being more common in the eastern states and Mexican heroin dominating the western ones.
Of note, different source countries and regions often produce distinct products, and this, too, is thought to be a contributing factor in regional differences in the timing of increased adulteration with IMF. While most of the world’s heroin—including that coming from Colombia—is a powder, Mexican heroin is a solid, dark-colored substance commonly referred to as “black tar.” These two distinct formulations of heroin have different purity ranges, may require different techniques for consumption, and are associated with different health risks.
Specifically, when IMF began its rapid rise in 2014, roughly three-quarters originated in the People’s Republic of China, and although the exact trafficking routes and strategies remain unclear, it would have been relatively easy to cut the white powder into the east coast’s supply of Colombian-sourced heroin. This led to the surge in fentanyl-adulterated or fentanyl-substituted heroin. Conversely, the black tar heroin that dominated western states’ opioid supply pre-IMF would have been far more difficult to mix with a powder. As such, IMF in the West took a different form—rather than being directly cut into the existing heroin supply, it more often entered the market as pills—and was slower to take off. In fact, most western states did not begin to experience fentanyl shock until after 2017. This rise in IMF proliferation coincides with Mexico’s rise to current dominance as the primary source country for the drugs.
It is noteworthy that, despite recent declines in overdose deaths, the illicit market continues to evolve. India is emerging as an IMF source country, and additional adulterants are constantly entering the market.
The Emergence of Xylazine
In 2019, Philadelphia, Pennsylvania, began seeing a surge in overdoses involving xylazine (also known as “tranq”), a powerful sedative commonly used in veterinary medicine. Although the drug has been a fairly common adulterant in Puerto Rico for at least 20 years, this was the first time it had been seen at such high levels and for so long in the continental United States. In 2020, xylazine was not among the top 25 drugs most commonly identified by the National Forensic Laboratory Information System, but within two years, it had become the 12th most commonly identified drug overall and the second most common tranquilizer or depressant. Similar trends have been observed in overdose data. Between January 2019 and June 2022, the percentage of monthly IMF-involved overdoses that also involved xylazine nearly tripled in 20 states and Washington, D.C., climbing from 2.9 percent to 10.9 percent. Consequently, in April 2023, the White House Office of National Drug Control Policy named fentanyl adulterated or associated with xylazine a national threat.
Understanding the emergence of xylazine as an adulterant once again requires a look at current drug use and supply contexts. Of particular relevance, the drug is found almost exclusively as an adulterant to IMF—roughly 98 percent of xylazine-involved deaths involve fentanyl—and, in some regions, the majority of IMF is now adulterated with the potent sedative. For example, in Maryland, drug-checking data from November 2021 through August 2022 found that 99.2 percent of opioid samples included fentanyl. Of the fentanyl-containing samples, 80 percent contained xylazine as well. Furthermore, as with IMF, xylazine’s proliferation has been geographically staggered, as seen in Figure 2. The drug first spread to several states in the Northeast, Midwest, and mid-Atlantic, where it remains the most prevalent. However, in 2022, “only three states reported zero xylazine seizures,” suggesting that this compartmentalization is unlikely to last.
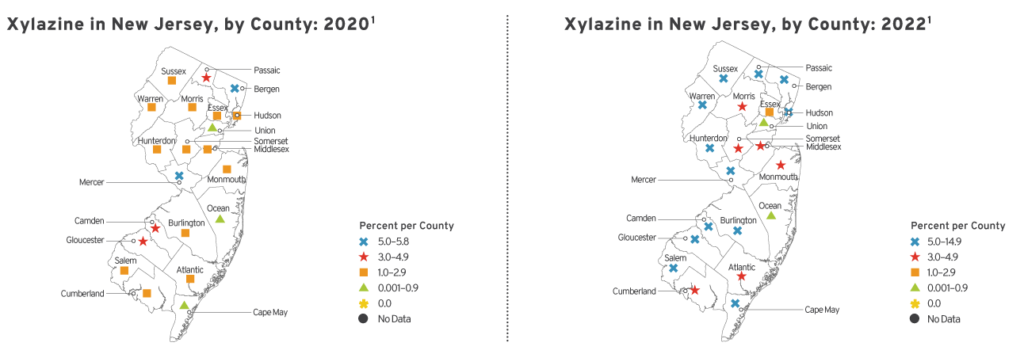
Furthermore, even within states, the emergence of xylazine and other adulterants can vary. For example, 2020 law enforcement seizure data from New Jersey showed that in some counties, almost 6 percent of reports contained fentanyl, whereas in other counties, that proportion was below 1 percent. Figure 3 maps the between-county variation in New Jersey in 2020 as well as showing the spread of xylazine across the state by 2022.
Figure 2: Percentage of Total Drug Reports Identified as Xylazine, by State, 2020 Versus 2022
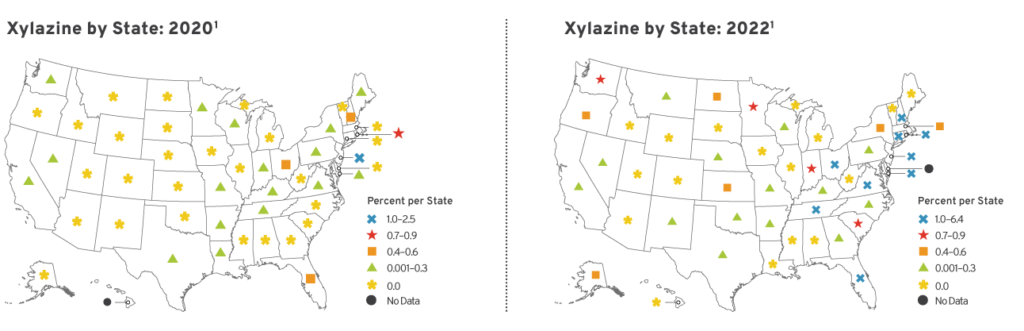
Figure 3: Percentage of Total Drug Reports Identified as Xylazine in New Jersey, by County, 2020 Versus 2022
As with IMF, evidence suggests that a demand-side push for xylazine on its own is extremely unlikely; numerous studies have found that the vast majority of PWUD do not want it, with many altering their consumption behaviors—for example, by smoking instead of injecting—and some actively seeking to avoid it altogether. The drug is highly sedating, complicates overdoses (it does not respond to the opioid overdose reversal medication naloxone), and is associated with an increased risk of necrotic soft-tissue injuries when injected—key factors that are cited by PWUD as reasons to avoid it altogether or change their consumption behavior. However, xylazine does have a perceived plus side for some PWUD, which may explain its “staying power” on the market now that it has arrived. Specifically, it extends the duration of the high people experience (fentanyl’s effects come on quickly but are very short-lived compared to heroin) and postpones withdrawal symptoms.
The Next Generation of Adulterants
As of the end of 2024, the U.S. illicit drug landscape is changing yet again. Total overdose deaths have been declining steeply for the past year, although some groups and some regions are continuing to witness a climb. Experts attribute much of this progress to the expansion of harm reduction, although shifts in supply may also have a role to play in some areas. While the decline in overdoses is certainly welcome, it does not mean lawmakers should stop prioritizing this issue. Past experience suggests that the drug supply will continue to change, driving the rise of yet more novel adulterants. Indeed, a close look at recent drug-checking data, drug seizures, overdose trends, and news reports from across the country indicates just that: The U.S. illicit drug supply is in flux.
Data from San Diego based on 4,348 law enforcement samples identified 52 adulterants, including nitazenes—a class of synthetic opioids several times more potent than fentanyl—and different classes of pharmaceutical sedatives. Other parts of the country have similarly identified an emerging mix of novel and known adulterants. Nitazenes have been seen sporadically throughout the country in recent years and have been responsible for overdoses in Colorado, Tennessee, Pennsylvania, and other states. In recent months, New York State’s Community Drug Checking Program has reported two to five samples per month that contain medetomidine (a novel potent sedative related to xylazine) as well as some samples containing dangerous combinations of opioids, xylazine, and benzodiazepines. Medetomidine has also been involved in overdose reports in Missouri, Colorado, Pennsylvania, California, Maryland, and Illinois. And drug-checking programs from Los Angeles to Delaware have seen an increase in BTMPS, an industrial chemical that is toxic to humans but does not cause overdose.
Arguably, this is just the beginning. As state and federal lawmakers play whack-a-mole with emerging adulterants—from misguided attempts to automatically schedule all fentanyl analogs to the push to criminalize xylazine—the drug supply will continue to evolve toward more unknown, often more potent, alternatives. These unknowns will continue to endanger our communities and loved ones. Thus, despite the recent promising reductions in overdoses, policymakers must continue to look for demand-side solutions that have been proven to save lives, such as harm reduction.
Harm Reduction Policy and the Evolving Supply
The overdose crisis has decimated communities for more than a decade, driving home the need for real solutions that help people stay as safe as possible in the face of an unregulated, illicit drug supply. More than 250,000 Americans have died of an IMF-involved overdose since 2018 alone, and more than 40 percent of Americans—an estimated 125 million people—have lost someone they know to a drug overdose. Other emerging adulterants may complicate or increase overdose risk, or they can cause severe secondary issues such as soft-tissue injuries, organ damage, gastrointestinal problems, cardiac issues, anemia, and more.
Changes in behavior can reduce some of these risks. However, when people are unaware of the contents or potency of their supply, they are less likely to know what steps are necessary to mitigate that danger. Harm reduction is a pragmatic approach that accepts the fact that some people engage in risky behaviors and thus prioritizes saving lives and supporting any positive change rather than exclusively promoting abstinence. Toward this end, harm reduction provides a range of tools that can help mitigate the potential risks associated with illicit substance use and the rapidly changing illicit drug supply. Rather than operating in opposition to or competition with abstinence- and recovery-oriented interventions, the approach provides an additional, lifesaving option to support efforts to combat the overdose crisis.
• Drug checking is a lifesaving intervention that tests small samples of an illicit substance for potentially harmful or life-threatening adulterants. Depending on state and local laws and the local context, drug checking may take several different forms. The most common drug-checking intervention in the United States is easy-to-use test strips that check for a single substance, usually fentanyl or xylazine, which are typically distributed by public health and harm reduction organizations. Another drug-checking option is point-of-service testing offered by public health and harm reduction organizations, which relies on a variety of test strips or more advanced technology such as Fourier-transform infrared spectroscopy to check for a wider variety of potential adulterants. Such community-based drug checking programs allow for more thorough testing and facilitate information sharing that can foster prevention.
Policy takeaway: Authorize drug-checking equipment broadly rather than substance-by-substance to allow frontline organizations to adapt quickly.
• Syringe services programs (SSPs) are community-based or public health organizations that distribute sterile injection equipment and collect used injection materials to protect communities by preventing injection-related diseases such as HIV and hepatitis C. However, they also serve as an important connection point for overdose prevention, distributing drug-checking equipment and naloxone, as well as providing overdose recognition and response training. In addition, SSPs connect their participants to a range of health and social services, including substance use disorder treatment resources. In fact, PWUD who engage with an SSP are four to five times more likely to engage in treatment than those who do not connect with such a program.
Policy takeaway: Authorize SSPs and allow sufficient flexibility for organizations to meet specific local needs.
• Naloxone has been an essential tool in combatting the current overdose crisis. This lifesaving medication is an opioid antagonist, meaning it binds to the same brain cells as intoxicating opioids such as heroin and fentanyl, and is able to push these other opioids off or prevent them from binding. To optimize the benefits of naloxone, it must be both widely available and affordable. Although some naloxone formulations are now available over-the-counter, SSPs and public health agencies remain the primary purchasers and distributors of the medication, especially to PWUD.
Policy takeaway: Continue to keep multiple formulations of naloxone accessible and affordable via naloxone-access laws and standing orders, and encourage overdose response by bolstering Good Samaritan Laws and liability protections for lay rescuers.
• Medications for opioid use disorder (MOUD) help reduce the number of people engaging with the unpredictable illicit drug supply. For example, the gold-standard MOUDs methadone and buprenorphine reduce withdrawals and cravings, helping people halt or reduce their use of illicit substances, and dramatically reduce overdose risk by up to 80 percent. However, buprenorphine is underprescribed, and methadone is hamstrung by overregulation and a monopolistic system of opioid treatment programs.
Policy takeaway: Expand access to methadone by reducing overregulation and allowing prescribing and pharmacy dispensing. Retain and continue to expand or improve on existing telehealth permissions for MOUD in accordance with recommendations from medical professional organizations such as the American Medical Association and American Society of Addiction Medicine.
Additional harm reduction interventions that have been implemented in other countries as well as in a handful of sites in the United States include overdose prevention centers and medical safe supply programs. While such programs remain controversial and technically illegal in the United States, evidence suggests that they can save lives or reduce other health-related harms when implemented with local challenges and individual patient or participant needs in mind.
Policymakers looking to combat the overdose crisis in their communities, especially in the face of an evolving drug supply, can work with local on-the-ground harm reduction and public health experts to ensure that legislation meets current best practices and allows for appropriate localized tailoring, flexibility, and real-time response.
Conclusion
In the United States, overdoses due to the illicit drug market have taken more than 1 million lives since 1999 and have cost the country roughly $1 trillion annually. In the past decade, the majority of these deaths have been attributable to the infiltration of potent synthetic opioids such as IMF. These drugs originally emerged as adulterants and over the years have come to dominate the illicit opioid supply. In more recent years, the drug supply has continued to shift, with the proliferation of the powerful veterinary sedative, xylazine, and the more recent emergence of novel synthetic opioids and sedatives. Even as overdose deaths fall, PWUD, the organizations that work with them, and the communities they live in must remain agile to prevent a resurgence or the rise of yet another crisis.
Harm reduction is a time-tested public health approach to mitigating the risks associated with illicit drug use and other potentially dangerous behaviors. Interventions such as naloxone access expansion and drug checking have likely played an important role in the current dip in overdose fatalities. And the approach will continue to be a fundamental tool in preparing communities to stay as safe and healthy as possible in the face of an ever-evolving illicit drug supply. However, to maximize the benefits of harm reduction in their communities, lawmakers must not only authorize the interventions, they must craft legislation that follows established evidence while allowing for tailored, adaptable programming that can address local challenges in real time.