
Maternal Health, Dissent, and Democracy: 100 Years After the Sheppard-Towner Act
“I wish I knew what mighty things were fabricating. If a form of government is to be established here, what one will be assumed? Will it be left to our assemblies to choose one? And will not many men have many minds? And shall we not run into dissensions among ourselves?“
—Abigail Adams writing to her husband, future President John Adams (1775)
In 1921, Congress passed a new law in response to high maternal and infant mortality rates. The law, which was called the Sheppard-Towner Maternity and Infancy Protection Act, provided modest funding to educate new mothers about caring for themselves and their newborns. The bill took several years to pass and was highly controversial. Some considered it a serious violation of privacy by the federal government, while advocates argued it was crucial to pass to prevent more mothers and babies from dying of a lack of basic hygiene practices. The debate itself wasn’t gendered; in fact, many women—including the only woman in Congress at the time—opposed the bill. But this isn’t a 100-year-old example of political dysfunction in America. Instead, the argument over who could (and should) improve maternal and infant health represents American democracy working exactly as it’s supposed to.
Maternal Health in the 1900s
Maternal and infant health outcomes were dismal in the early 20th century. In 1921, the U.S. Children’s Bureau reported that the United States ranked 17th among “civilized nations” in maternal mortality with 68 deaths per 10,000 live births. At the same time, 1 in 10 babies died before reaching one year old. State outcomes varied widely; even in 1934, South Carolina’s maternal mortality rate was as high as 87 (and Vermont’s rate as low as 39) per 10,000 births. For comparison, 2024’s maternal mortality rate was 17.9 per 100,000 live births.
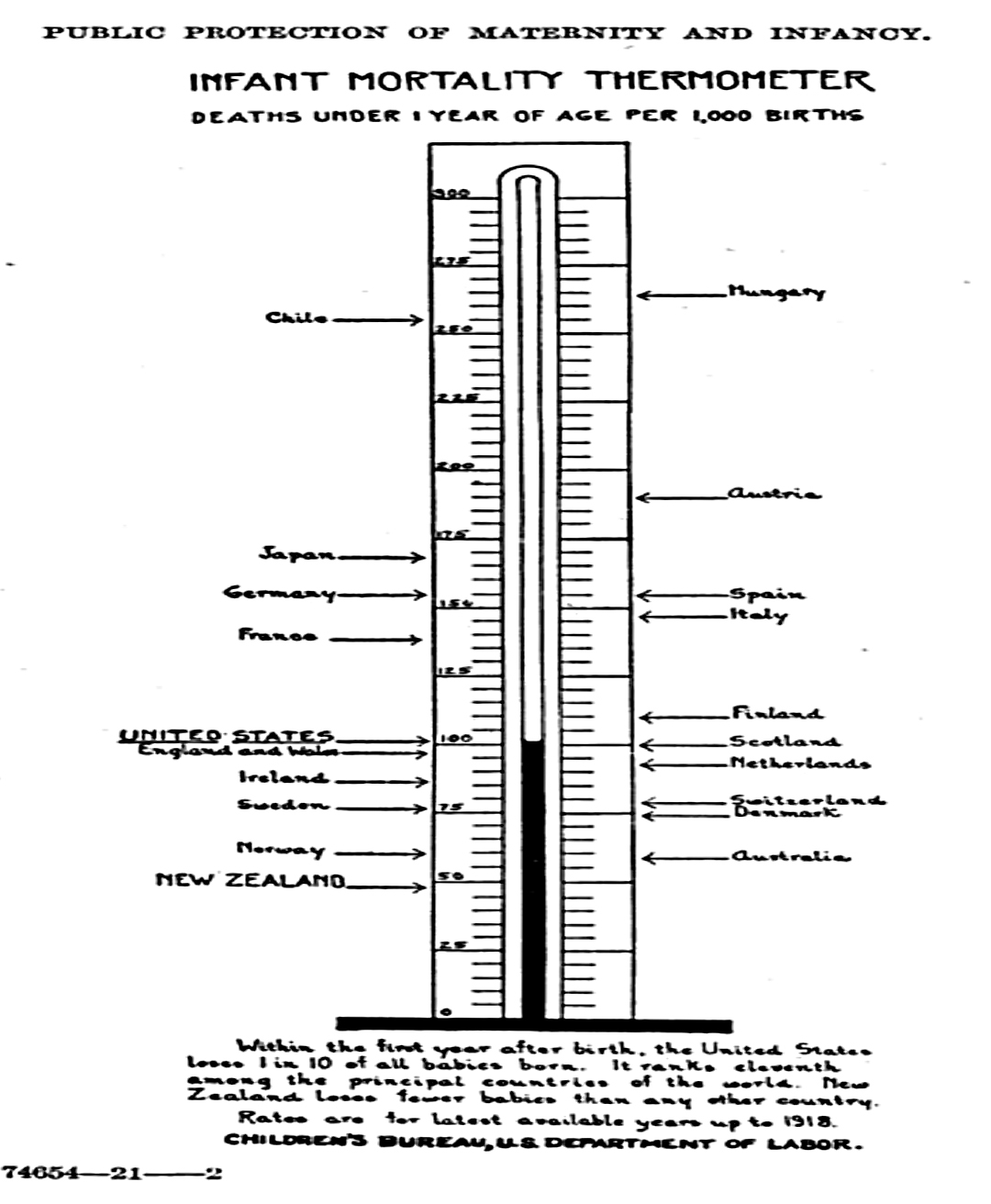
Graph presented in congressional hearings on the Sheppard-Towner Act (July 1921)
There were multiple reasons for this. First, general sanitation was lacking overall, and mothers often didn’t know how to remedy postpartum health problems or prevent infectious disease. Water filtration, pasteurized milk, and even understanding of bacteria weren’t yet widespread across the United States. In 1900, 40 percent of maternal deaths were due to sepsis. Later, the spread of basic hygiene practices like handwashing and glove-wearing would contribute critically toward the decline in U.S. maternal deaths.
Further, 80 percent of pregnant women in early 20th-century America received no formal prenatal care. A Wyoming woman wrote to the U.S. Children’s Bureau in 1916, expressing that “so many of my neighbors die at giving birth to their children” and pleading for the agency to send information about how to have her third baby without “being torn” in the process. Birth outcomes were especially dire for women who were poor, Black, or in rural areas. For example, in 1933, when the majority of Black women lived in rural areas, the infant mortality rate for babies born to Black mothers was twice as high as that of babies born to white mothers.
Even before women had the right to vote, women in powerful voluntary associations lobbied states for maternal aid. As a result, more states began looking for solutions. One example is New York’s Bureau of Child Hygiene, established in 1907, which provided education for new mothers in New York City’s crowded tenements and greatly reduced preventable infant deaths. In 1912, with pressure mounting for a federal response to maternal and infant health issues, Congress established the United States Children’s Bureau.
The Sheppard-Towner Act
The idea behind Sheppard-Towner was simple, at least in today’s terms. For five years, the federal government would disburse about $1 million annually in matching funds across states to use for things like sending nurses to counsel new moms and their babies; producing educational pamphlets on hygiene; and training midwives, who often worked in rural areas and played a pivotal role in the maternal health of Black women. U.S. Rep. Jeannette Rankin, a Montana Republican and the first woman ever elected to Congress, introduced a bill with this concept in 1917; however, it took a few years before the bipartisan team of Sens. Morris Sheppard (D-Texas) and Horace Mann Towner (R-Iowa) secured its passage.
The ratification of the 19th Amendment in 1920 had significantly changed the ways in which women influenced national politics. Perhaps unsurprisingly, getting the Sheppard-Towner Act passed was a high priority for some in this newly enfranchised group, many of whom had long complained about the state of maternal health.

Rep. Jeannette Rankin (third from right, front) and other women activists supporting the Sheppard-Towner Act
The Women’s Joint Congressional Committee—a large umbrella encompassing the League of Women Voters and other national women’s advocacy outfits—rallied other influential women-led groups to endorse the bill. The National Women’s Christian Temperance Union, the National Council of Jewish Women, the National Federation of Business and Professional Women’s Clubs, and others advocated for its passage. Maud Wood Park, president of the League of Women Voters, testified to Congress that childbearing was “an experience of paramount concern to women, we in whose hands the first responsibility for the conservation of human life has been placed. That is why a measure which is designed to save human life is a measure which must be of the most urgent concern to women.”
But women were not a monolith in thinking the federal government had a role to play. Plenty of women spoke out against the bill, as well. Rep. Alice Mary Robertson of Oklahoma, an antisuffragist and the only woman in Congress at the time, voted no. A common sentiment from women writing to Congress against the bill was that it violated their fierce sense of independence and privacy. This wasn’t necessarily a political stance; pregnancy was strictly women’s business at the time. As the National Museum of African American History and Culture notes, it was “taboo for a man to be present” during childbirth. Even when extolling the hardships that womanhood had brought them through births, deaths, and taking on labor while the men were at war, American women complained proudly. The Sheppard-Towner Act represented intervention into an extremely personal endeavor. In one statement of opposition, a Baltimore resident said, “Think of the embarrassment it would cause, should a prospective mother have to appear before the Public Health Board.”
Even some doctors were skeptical. One Harvard professor and leading OB-GYN wrote a letter to Congress in which he referred to the Act as “medical communism,” arguing that the federal government couldn’t do it as well as the private sector anyway. He said the medical field was already making steady progress in maternal and infant health and that “education of the people, guided by the medical profession, and the many altruistic societies devoted to human welfare” would best improve outcomes. (In other words, throwing federal dollars at the problem wouldn’t speed up the progress already taking place.)
Rep. Robertson also took a fiscally conservative line, arguing that states were already “overburdened with taxes” and that increased spending would hurt mothers more. The bill was law for several years before Congress purposely let its funding lapse (due in part to lobbying from the American Medical Association, who called it “socialized medicine” and said it undermined doctors’ authority).
Sheppard-Towner and 250 Years of American Governance
The debate over the Sheppard-Towner Act represents the best of America because to an extent, everyone involved was right. Maternal and infant mortality concerns deserved national attention, and state programs facilitating basic hygiene education deserved credit for improving outcomes. But there are always consequences to giving the government power over family affairs. Even during the time of Sheppard-Towner, multiple state-led child welfare programs were based in eugenicist thought about the ideal American family and often imposed those ideals on immigrants. Private-sector innovation did play a massive role in the historic decline of maternal and infant deaths—medical research was primarily funded by private/charitable funds into the 1930s, with federal funding almost nonexistent until World War II. During the Sheppard-Towner debate, everyone thought something should be done to improve maternal and infant health; they just vehemently disagreed about what could be done and who should do it.
It took all three—women’s advocacy, private-sector medical advances, and government investments—to sustainably drive down maternal and infant deaths. During debate over Sheppard-Towner, dissenting (and even unenfranchised) voices could still influence policy through voluntary association, open debate, and advocacy. What one group saw as helping moms and babies, others saw as imposing upon them. But that’s the point: The United States works best when dissent is allowed in the discourse.
James Madison saw dissent as a feature of our federalist system that would ultimately protect people from the whims of those in power. As he wrote in Federalist No. 51, “[T]he society itself will be broken into so many parts, interests, and classes of citizens, that the rights of individuals, or of the minority, will be in little danger from interested combinations of the majority.”
Abigail Adams worried we would run into dissent among ourselves about how to run the country; but fortunately, the American republic was meant to harness disagreement, not eliminate it. The Sheppard-Towner Act hearings show how dissent can ultimately shape policy by permitting serious debate among an array of interests. That’s a lesson worth remembering, 250 years later.