How Naloxone Co-prescriptions Affect Access and Overdose
Overdose is one of the United States’ greatest problems in recent history. More than one million people died of an overdose in the country over the last 20 years, and although the rate has finally slowed, over 150 people still die each day. The need to expand the application of innovative and effective solutions grows with every death.
One way policymakers have tried to reduce opioid overdose deaths is by encouraging or requiring doctors to prescribe naloxone alongside certain opioid prescriptions, especially for patients at higher risk. Naloxone is an opioid antagonist that reverses the effects of an overdose by displacing opioids from receptors, which restores breathing within minutes if administered promptly. The idea behind mandating naloxone co-prescribing is simple and logical: If an individual is receiving an opioid that carries a greater chance of overdose, then they should also have access to a medication that can reverse one. This post examines the impact of these policies.
Understanding Naloxone Co-prescribing
U.S. pharmacies dispensed more than 120 million opioid prescriptions in 2024. Though these medications are generally safe to take as prescribed and directed by a healthcare clinician, they are not entirely risk-free. More than 300,000 people died of a prescription opioid overdose in the United States over the last 25 years.
Those at greatest risk of overdose include:
- Individuals taking a high dose (≥90 morphine milligram equivalent)
- Patients prescribed opioids alongside other central nervous system depressants (e.g., benzodiazepines)
- Those who use opioid medications in a way other than as directed by their healthcare provider (almost 9 million people each year)
Despite the fact that prescription opioids come with some overdose risk, naloxone dispensing remains relatively low, with pharmacies dispensing only about 1.5 million prescriptions in 2024. Co-prescribing mandates aim to increase access to this lifesaving medication among individuals who take prescription opioids.
The Impact of Co-prescription Mandates
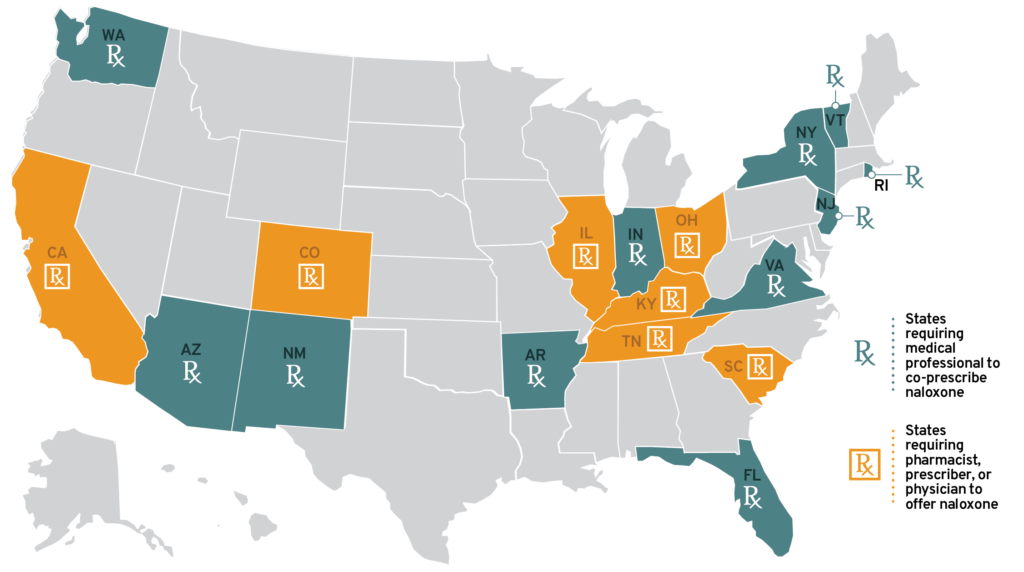
States began mandating that healthcare providers co-prescribe naloxone with opioid medications in 2018. As of May 1, 2024, 11 states required particular medical professionals to co-prescribe naloxone in certain situations; another seven required a pharmacist, prescriber, or physician to offer the medication.
State-level mandates were associated with significant increases in naloxone dispensing rates within months of being enacted. For example, a 2019 study found that states with these mandates dispensed naloxone at a rate approximately 7.75 times higher than states without such requirements. However, newer studies have come to mixed conclusions. First, not all states with co-prescribing mandates have seen significant increases in dispensing. Second, the increases are often short-lived, begging the question of whether these policies alone can drive sustained increases in dispensing. Furthermore, co-prescribing mandates do not appear to impact overdose death rates consistently in practice even if they increase naloxone dispensing. This may be because a relatively small number of people die from prescription overdoses versus illicit opioid overdoses. Given these inconsistencies in benefit and the fact that co-prescribing can increase the cost per prescription, it may not be appropriate to require naloxone co-prescribing for all opioid medications.
However, laws improving naloxone access and programs increasing naloxone distribution and overdose education are consistently associated with measurable reductions in opioid overdose mortality for people at high risk of overdose. Therefore, targeting co-prescribing mandates toward individuals prescribed high-dose and long-term opioids or other central nervous system depressants will likely benefit these at-risk individuals.
Conclusion
Naloxone co-prescription policies that focus on individuals at higher risk for overdose can be an effective part of a multi-faceted strategy to reduce opioid-related deaths, even if the policy only targets a small proportion of the population. By increasing access to a lifesaving medication among individuals at elevated risk, this approach improves the likelihood that naloxone is available when it is needed most and that its potential benefits offset cost-related concerns. However, naloxone co-prescribing is not a standalone solution. For population-level impact, naloxone co-prescribing should be paired with education, low-barrier non-pharmacy access, no-cost distribution to people who use illicit substances, and laws that protect lay responders.