Contraceptive Wants and Needs Among Women with Substance Use Disorders
About one-third of pregnancies in the United States are unintended, and that proportion almost triples to roughly 80 or 90 percent among women with a substance use disorder (SUD). Untreated SUD and unintended pregnancy each independently increase risk for a number of negative maternal and infant outcomes. Untreated SUD increases pregnant women’s risk of overdose, low infant birth weight, preterm labor, stillbirth, and more. Further contributing to these risks, the stigma associated with substance use during pregnancy can reduce the likelihood that a woman will engage with treatment or prenatal healthcare. The fact that most of these pregnancies are unintended only exacerbates the complications associated with pregnancy and an untreated SUD. These pregnancies are independently associated with a range of risks to mother and infant including maternal depression, intimate partner violence, preterm birth, and low birth weight.
Research shows that most women with an SUD want to avoid pregnancy and its associated risks, at least while they are grappling with chaotic drug use. However, only about one-third regularly use contraception compared to two-thirds of American women generally. Among women with SUDs, those who use contraception are most likely to use the least reliable methods, such as condoms, withdrawal and rhythm methods, and emergency contraception.
Given that most women living with an untreated SUD want to avoid pregnancy and its associated risks, policies must facilitate access to desirable and effective contraceptive methods. Understanding current barriers is essential to developing such policies.
Barriers to Contraceptive Uptake Among Women with an SUD
When we consider the problem of contraceptive uptake among women with an SUD, two outcomes leave room for improvement. First, a minority of these women regularly use contraceptives. Second, among those who do use them, only a minority use the most effective options: hormone pills and long-active reversible contraception (LARC) like implants or intrauterine devices (IUD).
Birth Control Tiers of Efficacy and Relative Uptake of Temporary and Reversible Contraceptives
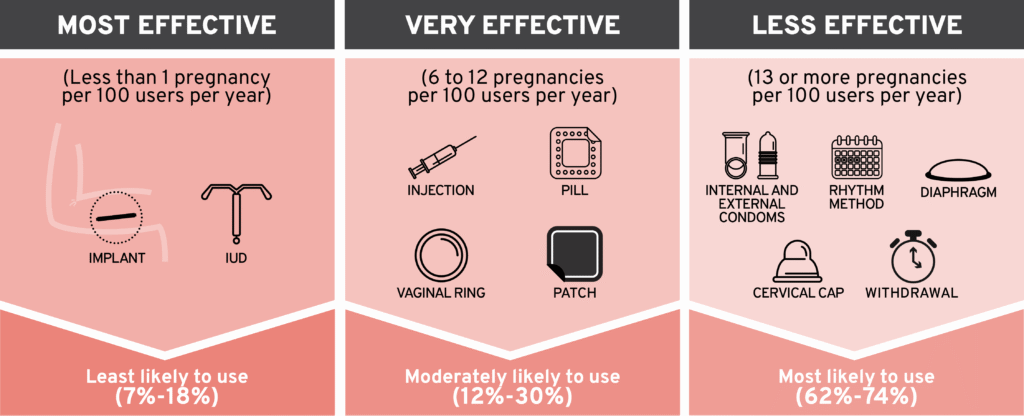
We must focus on eliminating barriers to these medical contraceptive tools. Research has identified contraceptive access barriers at multiple levels, from individual to societal. Some women avoid medical contraceptive options for personal reasons like religion, ambivalence about pregnancy, or a desire to avoid hormonal or invasive tools. Others may opt for barrier methods like condoms to prevent disease and are satisfied with this as their sole pregnancy prevention tool.
However, other women with an SUD are interested in medical contraceptives but unable to access them. People who use drugs—including women—often struggle to access medical care due to stigma and provider attitudes, lack of transportation and distance to care, provider shortages, and more. Cost is another important barrier that functions at multiple access points. Doctors and women alike cite insufficient insurance coverage and high out-of-pocket prices as major barriers to accessing providers as well as the contraceptives themselves. Fortunately, the right policies can improve access and choice.
{kind=link}
How Policy Can Improve Contraceptive Access for Women with an SUD
A smart policy environment will ensure low-barrier access to a variety of contraceptive options for women with an SUD, thereby increasing autonomy and control over their reproductive health and recovery journeys. Policies that address contraceptive cost and reduce healthcare system barriers when appropriate can improve both access and product choice while preserving women’s health. Here are a few examples:
- Annual Supply. State law typically allows women to access just 30, 60, or 90 days worth of short-acting contraceptives like the pill, patch, and ring; however, the “annual supply” approach allows pharmacists to dispense a full 12-month prescription of approved contraceptives. It has shown significant benefits, which include reducing unintended pregnancies and abortions, increasing the likelihood that women will stay on the medication after the first year, and reducing the need for emergency contraception. Not only does annual supply benefit women directly, the reduction in unintended pregnancies saves money for insurers and governments.
- Pharmacist Prescribing. Depending on the state, between 17 percent and 50 percent of American women lived in a “contraceptive desert” in 2018, with insufficient access to an affordable reproductive healthcare provider to dispense effective contraceptives. However, more than 95 percent of Americans live within 10 miles of a pharmacy, and people are about twice as likely to visit a community pharmacy as to see a doctor or other healthcare provider. Expanding pharmacists’ scope of practice to include prescribing birth control is one way to help improve access while maintaining women’s connection to the healthcare system. Research shows that this approach can improve medication uptake and adherence, especially for younger, less educated, and uninsured women.
- Over the Counter. Even pharmacist prescribing can be a barrier to care for some women with an SUD, especially if they are actively using and fear stigma or mistreatment. Over-the-counter (OTC) birth control provides a safe way for these women to protect their own health and control their reproductive life. Indeed, studies have found that OTC options increase contraceptive uptake and switching from less effective methods, disproportionately benefiting rural and uninsured women.
Policies that reduce physical barriers to contraceptives are only viable if women can afford the products. Given that reducing the number of unintended pregnancies saves women, insurers, and governments money, it makes financial sense for public and private insurers to cover a range of contraceptive products, including LARC. Beyond insurance, policies that allow health savings accounts (HSAs) and flexible spending accounts (FSAs) to cover nonprescription medications reduce out-of-pocket costs associated with OTC birth control. Approving additional contraceptive products for OTC status could also create competition to help drive down prices.
Conclusion
Like other American women, those living with an SUD want access to family-planning options. In particular, most do not want to become pregnant while they are in active addiction; however, they have high rates of unintended pregnancy and low rates of regular contraceptive use compared to the general population. Although women with an SUD face many barriers to accessing desired contraceptives, policies that address medical infrastructure and costs can have a major impact by reducing unintended pregnancies, supporting women’s autonomy, and saving everybody money.